
As a health professional dedicated to the well-being of young people, few topics weigh as heavily as the issue of first-time drug use, particularly when influenced by the powerful currents of peer pressure. It’s a complex landscape, often hidden beneath layers of adolescent development, social dynamics, and the pursuit of a sense of belonging. Understanding this intricate interplay is crucial for effective drug prevention for teenagers, equipping both young people and their support systems with the knowledge and tools to navigate these challenging waters.
The journey into drug use is rarely a solitary one. While individual vulnerabilities and pre-existing conditions can play a role, the initial step often occurs within a social context, where the desire to fit in, gain acceptance, or avoid social exclusion becomes a formidable force. Peer pressure, in its various forms, serves as a primary catalyst, subtly or overtly encouraging teenagers to experiment.
The Adolescent Brain: A Canvas for Influence
To truly grasp why peer pressure holds such sway, we must first understand the unique developmental stage of adolescence. The teenage brain is a work in progress, undergoing significant remodeling, particularly in the prefrontal cortex – the area responsible for impulse control, judgment, and risk assessment (Giedd et al., 1999). This means that while adolescents are increasingly capable of abstract thought, their ability to weigh long-term consequences against immediate gratification is still maturing.
Furthermore, the limbic system, associated with reward and emotion, is highly active during adolescence. This heightened sensitivity to rewards, coupled with a still-developing prefrontal cortex, makes teenagers particularly susceptible to the allure of novel experiences, excitement, and the perceived social benefits of fitting in with their peer group (Casey et al., 2008). The immediate “high” of acceptance or the thrill of breaking rules can easily overshadow the potential negative repercussions of drug use.
Deconstructing Peer Pressure: Beyond the Obvious
When we talk about peer pressure, it’s important to recognize that it’s not always a dramatic scenario of a bully forcing a younger teen to try drugs. Often, it’s far more subtle, insidious, and deeply ingrained in social interactions.
Direct Peer Pressure: This is the most recognizable form, involving explicit invitations or demands to try drugs. Examples include:
- “Everyone’s doing it, don’t be a square.”
- “Just one puff won’t hurt you.”
- “If you don’t try it, you can’t hang with us.”
While seemingly straightforward, the emotional weight behind these statements can be immense for a teenager desperate for acceptance. The fear of being ridiculed, ostracized, or seen as “boring” can be a powerful motivator to comply.
Indirect (Implied) Peer Pressure: This form is often more potent because it operates on a subconscious level, leveraging a teenager’s desire to conform and belong.
- Observational Learning: Teenagers observe their peers using drugs and perceive it as “normal” or “cool.” They may then internalize the belief that drug use is a prerequisite for social acceptance within that group.
- Perceived Norms: Adolescents often overestimate the prevalence of drug use among their peers. This “false consensus effect” leads them to believe that “everyone is doing it,” creating pressure to conform to what they perceive as the norm, even if it’s not the reality (Perkins & Berkowitz, 1986).
- Modeling Behavior: When popular or influential peers engage in drug use, it can set a precedent that others feel compelled to follow to maintain their social standing or emulate those they admire.
- Fear of Missing Out (FOMO): Social media amplifies this. Seeing photos or stories of peers engaging in drug-related activities can create a sense of exclusion and a fear of missing out on “fun” experiences, pushing teens towards similar behaviors.
Internalized Pressure: Perhaps the most challenging form of peer pressure stems from within. A teenager might anticipate negative social consequences if they refuse drugs, even without an explicit threat. This internal monologue, driven by self-doubt and a strong desire for acceptance, can be as powerful as any external demand.
Why Teenagers Succumb: A Web of Vulnerabilities
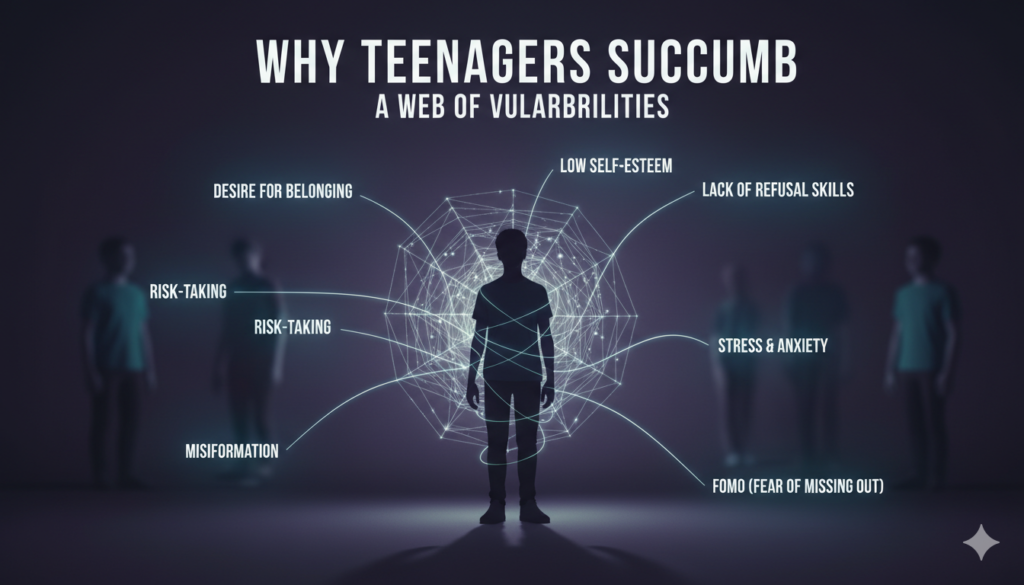
Several factors make teenagers particularly susceptible to peer pressure regarding drug use:
- Desire for Belonging and Acceptance: Adolescence is a critical period for identity formation, and peer groups play a pivotal role. The need to belong, to be accepted, and to feel connected is profoundly strong. Refusing drugs when offered by friends can feel like a rejection of the group itself, risking social isolation.
- Developing Sense of Self: While striving for independence, teenagers are also figuring out who they are. They may lack a strong sense of self-identity and firm personal boundaries, making them more easily swayed by external influences.
- Risk-Taking Propensity: As mentioned, the developing adolescent brain is hardwired for novelty and risk-taking. Experimenting with drugs can be perceived as an exciting, rebellious act that provides a thrill and a sense of maturity.
- Low Self-Esteem: Teenagers with low self-esteem may be more vulnerable to peer pressure, as they are more likely to seek external validation and acceptance. They may believe that conforming to drug use will make them more likable or popular.
- Lack of Refusal Skills: Many teenagers simply haven’t developed the confidence or communication skills to effectively refuse drug offers without feeling awkward or fearing repercussions. They might struggle to articulate a clear “no” or suggest alternatives.
- Misinformation and Glorification: Despite widespread prevention efforts, misinformation about drugs persists. Teenagers may underestimate the risks, believe in myths about certain substances being “safe,” or be influenced by media portrayals that glamorize drug use.
- Stress and Emotional Dysregulation: Adolescence can be a period of significant stress – academic pressure, family conflicts, romantic challenges, and body image concerns. Some teenagers may turn to drugs as a misguided coping mechanism, especially if they see peers using substances to manage their emotions.
The Alarming Connection: Peer Pressure to First-Time Use

Numerous studies confirm the strong link between peer influence and the initiation of drug use. Research published in the Journal of Studies on Alcohol and Drugs has consistently shown that having friends who use substances is one of the strongest predictors of an adolescent’s own substance use (Dishion & Loeber, 2003). The pathways are clear:
- Increased Exposure: Being part of a peer group where drug use is prevalent naturally increases a teenager’s exposure to drugs and the opportunities to try them.
- Normalization of Behavior: When drug use is common within a social circle, it becomes normalized. The perception of risk decreases, and the behavior is seen as acceptable, or even expected.
- Pressure to Conform: The explicit and implicit pressures discussed earlier culminate in the decision to try drugs for the first time. This initial step is often driven less by a genuine desire for the drug’s effects and more by the social imperative.
Effective Drug Prevention for Teenagers: A Multifaceted Approach
Given the powerful influence of peer pressure, effective drug prevention for teenagers must be comprehensive, proactive, and involve multiple stakeholders.
1. Fostering Strong Family Connections:
- Open Communication: Parents are the first line of defense. Establishing an environment of open, non-judgmental communication where teenagers feel safe discussing challenges, fears, and temptations is paramount. Regularly discussing the risks of drug use, without lecturing, can be highly effective. (National Institute on Drug Abuse, 2020).
- Setting Clear Expectations and Boundaries: Consistent rules and consequences, coupled with genuine warmth and support, provide a stable framework. Teenagers need to know where their parents stand on drug use and understand the repercussions of engaging in such behaviors.
- Active Engagement: Being actively involved in a teenager’s life – knowing their friends, hobbies, and where they spend their time – allows parents to identify potential risk factors and intervene early.
- Role Modeling: Parents who model healthy coping mechanisms, stress management techniques, and abstain from substance abuse themselves set a powerful example.
2. Equipping Teenagers with Resilience and Refusal Skills:
- Building Self-Esteem and Self-Worth: Programs that help teenagers develop a strong sense of self-worth and confidence can empower them to resist negative peer influences. When a teenager values themselves, they are less likely to seek external validation through risky behaviors.
- Assertiveness Training: Teaching practical refusal skills – how to say “no” firmly and confidently, how to change the subject, or how to suggest alternative activities – is crucial. Role-playing these scenarios can be highly effective.
- Critical Thinking and Media Literacy: Helping teenagers critically evaluate information, challenge perceived norms, and recognize manipulative tactics in advertising or social media can arm them against misleading portrayals of drug use.
- Stress Management and Coping Skills: Providing healthy outlets for stress, such as exercise, mindfulness, hobbies, or seeking support from trusted adults, reduces the likelihood of turning to drugs as a coping mechanism.
3. Empowering Positive Peer Influence:
- Promoting Healthy Peer Groups: Encouraging involvement in structured, positive activities like sports, clubs, volunteer work, or faith-based organizations can connect teenagers with peers who share similar values and goals, reducing exposure to drug-using environments.
- Peer Mentoring Programs: Older, positive role models can be incredibly influential. Peer mentoring programs can provide guidance, support, and demonstrate healthy choices.
- Social Norms Campaigns: Correcting misperceptions about the prevalence of drug use among peers can be highly effective. Campaigns that highlight the fact that most teenagers do not use drugs can reduce the perceived pressure to conform (Montana Social Norms Project).
4. School-Based Prevention Programs:
- Evidence-Based Curricula: Schools play a vital role in providing comprehensive drug education that is age-appropriate, evidence-based, and ongoing. Programs like “Project ALERT” or “LifeSkills Training” have demonstrated effectiveness in reducing substance use among adolescents (Botvin & Griffin, 2004).
- Safe and Supportive School Environment: A school culture that prioritizes student well-being, fosters positive relationships, and provides accessible mental health support can act as a protective factor against drug use.
- Teacher Training: Equipping educators with the skills to identify signs of substance abuse, address peer pressure dynamics, and refer students to appropriate resources is essential.
5. Community-Wide Initiatives:
- Accessible Mental Health Services: Addressing underlying mental health issues like anxiety, depression, or trauma can significantly reduce the risk of self-medication with drugs. Ensuring accessible and affordable mental health services is critical.
- Limiting Access: Community efforts to limit the availability of drugs, such as strict enforcement of age restrictions for alcohol and tobacco, and addressing the illegal sale of prescription drugs, contribute to prevention.
- Public Awareness Campaigns: Broad campaigns that educate the community about the dangers of drug use, the signs of substance abuse, and available resources can create a supportive environment for prevention.
Recognizing the Warning Signs: When to Seek Help
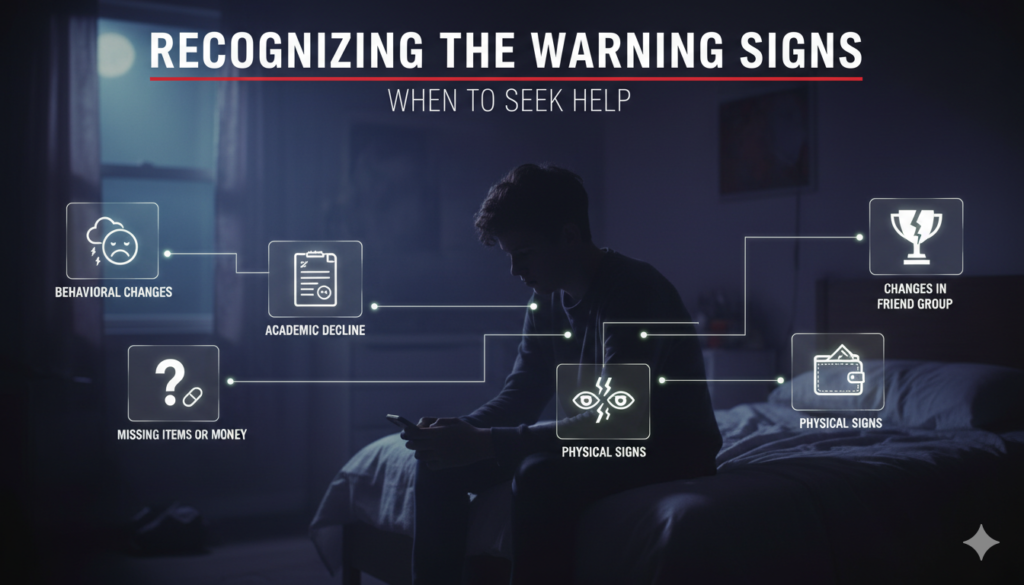
Despite the best prevention efforts, some teenagers may still experiment with or develop a reliance on drugs. It’s crucial for parents, educators, and other adults to be aware of potential warning signs:
- Behavioral Changes: Sudden changes in mood (irritability, hostility, depression), secrecy, withdrawing from family activities, lying, or neglecting responsibilities.
- Academic Decline: A noticeable drop in grades, missed assignments, or disciplinary problems at school.
- Changes in Friend Group: New friends who are unknown or seem to have a negative influence.
- Physical Signs: Bloodshot eyes, dilated pupils, changes in sleep patterns, appetite changes, poor hygiene, or unexplained weight loss/gain.
- Missing Items or Money: Unexplained disappearances of money, prescription medications, or valuables.
- Loss of Interest: Losing interest in hobbies, sports, or activities they once enjoyed.
If you observe these signs, it’s essential to approach the situation with concern, not accusation. Open a dialogue, express your worries, and seek professional help from a doctor, school counselor, or addiction specialist. Early intervention is key to preventing casual experimentation from escalating into a serious problem.
Conclusion: A Collective Responsibility
The journey through adolescence is fraught with challenges, and peer pressure to use drugs is undeniably one of the most significant. As health professionals, parents, educators, and community members, we share a collective responsibility to create an environment where young people feel empowered to make healthy choices. By understanding the intricate dynamics of peer pressure, fostering strong relationships, equipping teenagers with essential life skills, and implementing comprehensive prevention strategies, we can significantly reduce the rates of first-time drug use.
Drug prevention for teenagers is not a one-time conversation; it’s an ongoing commitment to nurture resilience, promote well-being, and guide our young people towards a future free from the grip of substance abuse. By working together, we can help them navigate the storm and emerge stronger, healthier, and more empowered to live fulfilling lives.
References:
Botvin, G. J., & Griffin, K. W. (2004). LifeSkills Training: Empirical findings and future directions. Journal of Primary Prevention, 25(2), 211-231.
Casey, B. J., Jones, R. M., & Hare, T. A. (2008). The adolescent brain: Changes in structure, function, and connectivity. Trends in Cognitive Sciences, 12(12), 473-479.
Dishion, T. J., & Loeber, R. (2003). Adolescent marijuana use: A review of the literature on risk and protective factors. Journal of Studies on Alcohol and Drugs, 64(6), 803-818.
Giedd, J. N., Blumenthal, J., Jeffries, N. O., Castellanos, F. X., Liu, H., Zijdenbos, A., … & Rapoport, J. L. (1999). Brain development during childhood and adolescence: A longitudinal MRI study. Nature Neuroscience, 2(10), 861-863.
Montana Social Norms Project. (n.d.). Retrieved from [You would insert a specific URL if available, or state generally if it’s a known project].
National Institute on Drug Abuse. (2020). Parents: Facts for teens and parents. Retrieved from [You would insert the specific NIDA URL for this resource].
Perkins, H. W., & Berkowitz, A. D. (1986). Perceiving the community norms of alcohol use among students: Some implications for student alcohol abuse prevention. International Journal of the Addictions, 21(9-10), 961-973.


